










The Haredim who break out of their bubbles to join the IDF are often caught between faith, family and country. Here are some of their stories.
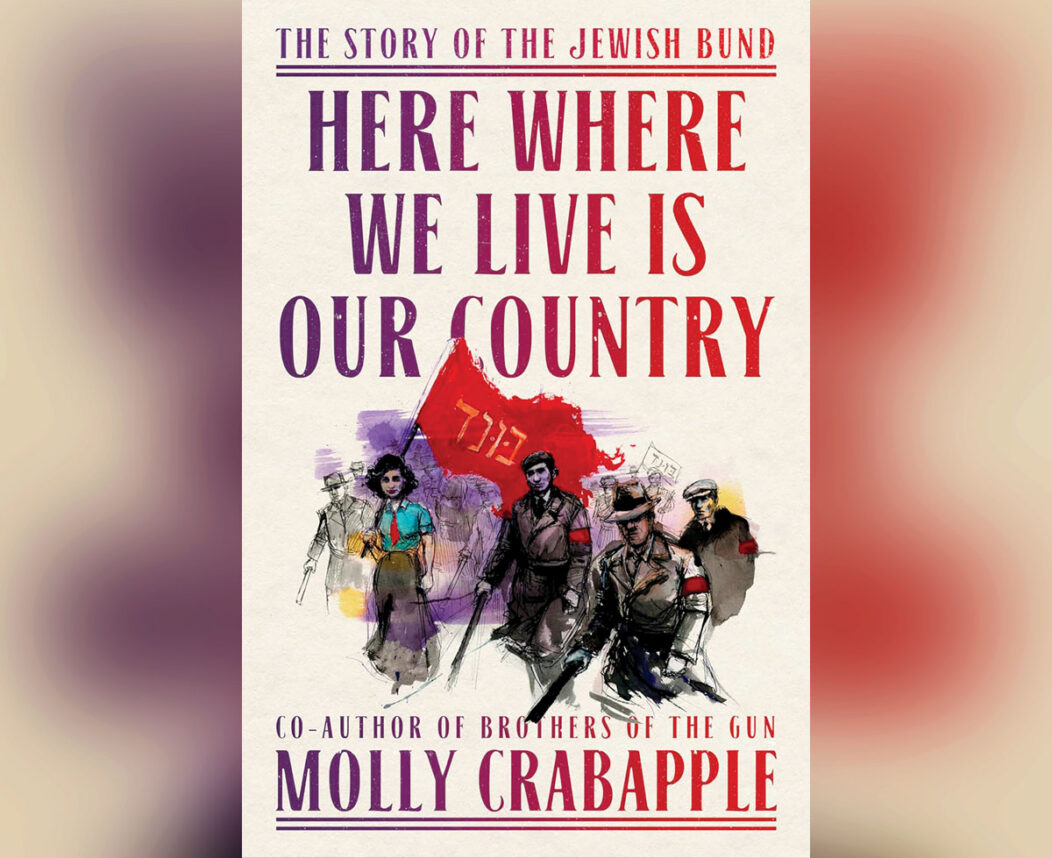
Molly Crabapple has written a work of great inversion and of ultimate betrayal.

For the director/artist, creating images inspired by Torah is a way of engaging with the stories, ideas and interpretations that have shaped Jewish life for thousands of years.

I took three different dates, ages 6, 72 and 35, to see Dataland, the unusual digital art experience in downtown Los Angeles.

This is the transcript of the speech Rabbi Dr. Bradley Shavit Artson gave at the 2026 AJU Gala on May 19, 2026.

A classic Australian dessert chocolate coconut slice features a rich, dense, fudgy chocolate base packed with dried coconut, finished with a thick cocoa frosting and generously dusted with even more coconut.

This roundup has recipes from two matchmakers: one is perfect for a special date night, the other is the perfect representative of lasting love.
Secret Sauce

For decades, the question of Haredi enlistment has remained one of Israel’s most sensitive and unresolved conflicts.

At the very least, the case would provide a global stage to debunk the genocide lie that is devastating world Jewry.

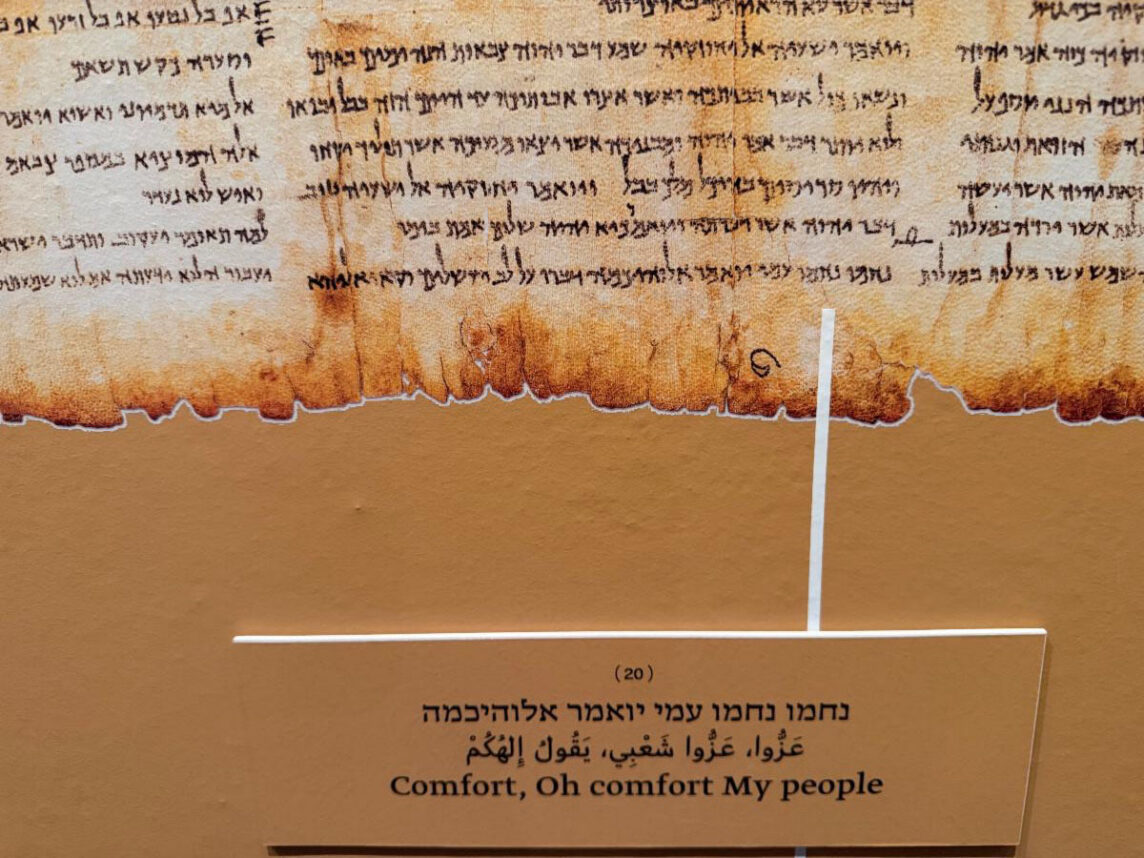
This Tisha b’Av, as we mourn over the Temple once more, it is an occasion to consider what resonance the remnants of the Temple structure hold for us today.

Coalition supporters want to define Eisenkot as a leftist because leftist is a title most Israelis do not want their Prime Minister to hold. But this definition has inherent limitations.

Last week, I moderated a panel of interfaith leaders fighting antisemtism and supporting Israel as part of the American Muslim and Multifaith Women’s Empowerment Council’s conference.

As if life needed one more complication, my anniversary with life, my birthday, usually falls somewhere inside the Three Weeks, that narrow corridor of Jewish time when celebration starts to feel suspicious.

Does Morocco have genuine warmth toward Jews, or is it a way to reignite lucrative Jewish tourism? Does it even matter?


Anti-Israelism has become a kind of cultural and political loyalty test that has almost nothing to do with the actual policy questions at stake. If the postwar liberal order is fragmenting, the story of Israel is a symptom of that fragmentation, not its cause.

The film reminded me that an ancient poet could write about massacres but also about moral courage, while terrorists who dream of killing Jews can only think of going right to the massacre.





